QUESTION
1. RESEARCH PROPOSAL FORMAT
2. Title of Paper (12-25 Words)
Health Seeking Behaviour with Special Reference To Epidemic Acute Watery Diarrhoea (Awd) In Somali Region Of Ethiopia
3. Abstract (Up to 300 Words)
The researcher intends to evaluate the role played by family practices in promoting behaviours (practices, attitudes, beliefs, and social norms) that prevent risk of cholera/AWD transmission and explores contextual factors that shape treatment-seeking in the 1st 90 days of interventions. Objectives are based on the role of behaviours of family practices i.e. attitudes, beliefs and social norms as primary factors that influence AWD outbreak; on the basis of its uniqueness in climatic conditions as compared to other areas of the Republic of Ethiopia. The other socio-economic, political and demographic issues to be considered as factors that enhances the spread of the disease and or support treatment seeking. The study intends to use a triangulation of qualitative and quantitative approaches. Data will be collected from the five zones (Jijiga, Jarar, Dollo, Shabelle and Fafan) of Somali region of Ethiopia. Thiswill be a case study selected randomly from the republic of Ethiopia Somali region and sub Saharan Africa. The data analysis will be done using statistical correlation analysis technique to investigate the relationships between the different variables that came up as important factors in the spread of cholera and prevention. The collected data will be primary and secondary data. This will be collected using questionnaires, interviews, observations, and set reading of published materials on Acute Watery Diarrhea (AWD).
From the literature, it is clear that public health primitive interventions is a catalyst to avert disease outbreaks (AWD), however, in the sub Saharan countries, this reality is far. Hence, the need for research that will provide an understanding of what should be done differently to make them a success story especially in countries where the health sector has not achieved the health care universal coverage and are still facing multiple disease outbreaks.
4. Research Objectives (Around 25 Words)
The study aims to evaluate the role played by family practices in promoting behaviours that shape prevention and treatment seeking in the 1st 90 days of AWD intervention.
5. Identification/Defining Research problem (No word count)
A wide gap in knowledge regarding hygiene family practices has lead to outbreak of Cholera/AWD in many sub-Saharan parts of Africa. The outbreak has been unpredicted and have spread upto Somali region of Ethiopia and Moyale. The situation remains unchanged even in presence of various medical conditions. The main research questions of the research are as follows:
-
What is the role of family practice regarding spread of AWD/Cholera in Somali region of Ethiopia?
-
What are the various factors that lead to rampant transmission of AWD among adults aged 15-49 in Somali region of Ethiopia?
-
What are the various behavioural, social and cultural attributes within this region that aids in prevention and treatment of AWD/Cholera?
-
What are the recommendations that can be made regarding interventions implemented by Government, NGOs and stakeholders for the treatment and prevention of AWD/Cholera?
6. Thesis Statement/Hypothesis (No word count)
Can the use of a combination of biomedical, behavioural, environmental, and treatment seeking strategies reduce barriers to AWD testing and improve prevention cascade among adults aged 15-49 years in the Somali region of Ethiopia.
7. Literature Review (No word count)
PICO STATEMENT
-
-
-
Search Strategy
-
-
Keywords improve specificity and credibility of research being conducted (Peachey, Hall and Cegielski 55-69). Various keywords will be used for obtaining relevant literatures in accordance to the topic. Some of the keywords that will be used includes Cholera/AWD outbreak; AWD testing and counselling, Family practices, behaviours, Adults, and Somali region of Ethiopia. The MESH terms that will be used for research include AWD, diagnosis, prevention, adults. Various databases will be searched for obtaining appropriate literature. Some of the databases include Google Scholar, PubMed and PubMed Central. Boolean search strategy will be used using AND/ OR as outlined below:
|
KEYWORDS |
AND/OR |
KEYWORDS |
AND/OR |
KEYWORDS |
|
AWD* |
AND |
AWD testing |
OR |
AWD family practices * |
|
AWD family practices* |
OR |
AWD behaviours |
OR |
AWD diagnosis* |
|
AWD diagnosis |
AND |
AWD Counselling |
AND |
Adults |
|
AWD Counselling* |
AND |
Adults |
AND |
Somali region of Ethiopia |
|
AWD testing |
OR |
AWD diagnosis* |
AND |
AWD family practices |
Table 1: BOOLEAN search strategy to be used
-
-
-
Literature search
-
-
Several Suitable peer reviewed qualitative and qualitative studies regarding AWD prevention and treatment for 15-49 years adults will be analysed. Moreover studies reporting AWD prevalence in Somali region and whole of Ethiopia, East Africa, Sub-Saharan Africa and Asia will be collected from several databases such as PubMed, PubMed Central and Global Health. Articles that were published after 1970, that is after the break out of the disease will be studied. Furthermore, additional studies will be sorted from both the reference and related citation lists next to the PubMed summary list. Official WHO, CDC, UNICEF, UNHCR, UHI and UNAIDS sites, and National Government Agency sites and reports will be thoroughly searched. However, one of the national reports included was in Ethiopia due to its high relevance. 2,640 peer-reviewed articles and reports will be identified for further screening.
7.1.2 Inclusion and exclusion criteria
The inclusion and exclusion criteria will be used for analysis of relevant data. Setting up of exclusion and inclusion criteria adds to specialist of research and ensures progress of data in a definite direction (Lewis 473-475). The search process gets narrowed down and journals with irrelevant data are exclusive. The inclusion and exclusion criteria are enlisted within following table:
|
Inclusion Criteria |
Exclusion criteria |
|
● Target population (adults 15-49 years) ● Presence of proper experimental methodology ● Presence of systematic review of literatures within journals with evidences ● Availability of statistical data ● Authentic and peer reviewed journals
|
● Individuals younger than 15 years and older than 49 years ● Lack of literature review and evidences ● Lack of credible sources regarding data within journals ● Lack of statistical information ● Non peer reviewed journals
|
Table 2: Inclusion and Exclusion criteria
(Source: Influenced by Lewis 473-475)
Intervention group
Participants will receive health education and sensitization based on the use of a combination of biomedical, behavioural, environmental, and home-based testing strategies. The first educational session will be delivered after collection of baseline data. The impact of the intervention on the study outcome variables will be evaluated at 12 months.
-
-
Acute Watery Diarrhoea/ Cholera:-
-
Drought, famine and cholera/AWD (Acute Watery Diarrhoea) outbreaks have become recurrent in the Horn of Africa (WHO 2017). Somali region of Ethiopia is no exception. Drought naturally contributes to trigger increases in epidemics such as AWD and measles, some of which are cross-border outbreaks (UNHCR 2017). AWD remains a significant public health problem in many parts of Somali region of Ethiopia, where they can spread quickly unless an outbreak is stopped. This underpins the international partners evidence on humanitarian responses to AWD in Ethiopia, in terms of necessary cross district and/or cross border co-ordination, as well as the human and financial resources needed (Fisseha, 2016; Oxfam GB, 2017; UNICEF, 2017a; OCHA Somalia, 2018). WHO (2017a; 2017b; 2018; Fisseha, 2016), UNICEF (2017a, 2017b; Beauregard, 2017) and Oxfam (2017) have assessed their own AWD responses in Ethiopia and neighbouring countries. In developing countries, up to 50 per cent of cases die from dehydration and kidney failure, if not adequately rehydrated. Infection without symptoms or with only mild diarrhoea also occurs, particularly in children (UNICEF 2016).
AWD outbreaks in Somali region are often cyclical and manmade causing substantial morbidity and mortality (UNICEF 2016). While there are some contextual and environmental factors involved, such as decreased rainfall and decreased vegetation cover, the conflict and poor family practices is the main driver of the outbreaks (UNICEF 2017). This can be complex with limited water access, latrine use and food handling practices for AWD prevention and treatment seeking. Outbreaks of diarrheal disease, including AWD/cholera, further worsen the situation of ongoing drought and conflict (US Department of State Humanitarian Information Unit (HIU 2017).This can be as a short outbreak and protracted epidemic. The transmission of the causative bacteria is usually through the faecal-oral route of contaminated food and or water caused by poor sanitation practices (UNICEF 2017).
AWD are contagious waterborne diseases that are transmitted through Vibrio cholerae. The disease is highly contagious and is transmitted mainly through purified drinking water and often by undercooked seafood (WHO 2016). Symptoms may appear as soon as within few hours to as long as five days. The main symptoms include large volumes of fluid loss through watery diarrhoea, often termed as ‘rice water stools’, vomiting, leg cramps, circulatory collapse and shock. Fatality occurs within 25-50% of the cases in absence of proper treatment (CDC 2016). It kills within short time, if patients are not rehydrated and given adequate mineral and liquid balance needed in human body. The risk increases at epidemic proportions in regions with poor water and sanitation facilities, lack of health facilities, poverty-stricken areas, overcrowding, drought, conflicts, insecurity, and uncontrolled areas of water sources.
In 2016, WHO and its partners, acknowledged the continued public health threat posed by the disease; the enduring problems of lack of access to clean water and adequate sanitation; and the absence of any long-term impact on cholera incidence through perennial responses to major outbreaks. Mass urbanization, climate change, and growing competition for water resources may, in fact, contribute to further increases in the AWD burden (WHO 2016).
7.2 AWD spread in the region (Kenya and Ethiopia)
From late 2014 to end of 2015, AWD outbreak has seized 30 of the 47 counties of Kenya causing close to 7000 cases of morbidity and over 100 deaths. The outbreak occurred in light of the El Niño floods which created favourable conditions for the spread of the causative bacteria. After spreading in Kenya for over a year, the disease moved to Ethiopia.
In Ethiopia, AWD was first reported in districts of Oromia and Ethiopian Somali close to the Ethio-Kenyan border (Moyale) in February 2016. Thereafter, it continued spreading east and north reaching many parts of the country including the capital city and the northern parts of the country and Somali region of Ethiopia remain the hardest hit due to several reasons. Despite an ongoing effort to contain the outbreak, it continued spreading to large areas of the country affecting a large number of people; its course remained protracted and kept many people at risk.
The Cholera/AWD risks factors that propagated the spread of the disease are:
-
Water, Sanitation and family practices: Insufficient WASH access, population density, poor awareness about the disease and way of life. Violence prevents people from accessing adequate water sources, displaces them to settlements with poor water and sanitation and hinders them reaching health care centres. In addition, in a drought, water becomes scarce and pathogens accumulate in stagnant waters, and people and cattle are pushed to use these contaminated waters, sharply increasing the risk of a cholera/AWD epidemic.
-
Demographic and social factors: Demographic explosion especially in big cities-associated with poverty and disordered urbanization is a key factor in the occurrence of the outbreak. Big gatherings (pilgrimages and celebrations), communal eating practices, that favour overcrowding and lack of hygiene practices at family level are risk factors that exacerbate the outbreak.
-
Climatic condition (Famine, drought): AWD outbreak is known to occur in humid and inter-tropical zones during rainy seasons. Flooding during rainy seasons can favor the emergence or the upsurge of AWD outbreak. Although the causative bacteria are more delicate in the atmospheric environment than in its aquatic environment, it can survive well for days on fruits and vegetables. Ecosystem changes due to global warming, environmental pollution, drought, deforestation leading to floods and other climatic disasters are the reason for the upsurge of AWD outbreak.
7.3 Gaps in Knowledge and how this will inform my Research Project
There are several literatures regarding identification of interventions regarding AWD testing and treatment seeking strategies. In the present context there exists a profound lack of knowledge regarding family practices that promotes assistance seeking behaviours in 1st ninety days of AWD interventions. Moreover, most of the studies were conducted in Asia, USA and Haiti where the prevalence of disease is completely different from that of Somali region of Ethiopia. The current research shall focus on promotion of awareness strategies and not confine itself to coping and behavioural risk reduction programmes. In addition, there exists a gap in knowledge regarding nutritional services and clinical trials conducted for finding treatment protocols of AWD/Cholera. There is a need of research focusing on prevalence and interventions methods specified towards Somali region of Ethiopia in order to promote better health status among people.
Some studies presented in media newsletters and blogs were excluded because of limited credibility of source and missed out approaches that lead to promoting good family practices for AWD services. In general, most gaps that have been identified with the studies are that they did not discuss further, intervention strategies but rather mentioned them broadly. Most of the studies/reviews conducted were outside Somali region of Ethiopia a gap that indicated limited study of AWD on family practices in this setting. With this background, there is need for more studies to assess the role played by family practices in promoting behaviours that shape prevention and treatment seeking in the 1st 90 days of AWD intervention.
8. Research Methodology (No word count)
Within this research triangulation approach will be used. Both qualitative and qualitative approaches will be used. However, substantial amount of information will be collected through qualitative analysis of articles. The process will allow the research to be flexible in nature while maintaining its specificity towards fulfilment of its objectives (Jentoft and Olsen 147-170). The data regarding prevalence of data will be collected from both adults belonging to age group 14-49 years of age. In addition five areas will be used for collecting data namely Jigjiga, Jarar, Dollo, Shabelle and Fafan of Somali region in Ethiopia. The sampling technique for research subjects will be randomly sampling selected from the affected zones. The data analysis will be done using correlation analysis technique. The collected data will be primary and secondary data and the data will be collected using questionnaires, interviews, observations, and set reading of published research material including both present and historical information on disease outbreaks, mainly Acute Watery Diarrhea (AWD) sometimes known as Cholera.
8.1. Research design
Study Design
Type of study
A cluster sampling will be designed (qualitative , quantitative, comparative, and analytical in nature) to assess the role played by family practices in promoting behaviours that shape prevention and treatment seeking using a combination of health education strategies (intervention) on AWD testing and sustaining good family practices among adults aged 15-49 years in five (5) communities. This will be compared to Standard care seeking (control) in five (5) communities all in the Somali region of Ethiopia. The study will involve evaluating the outcome of a combination of biomedical, behavioural, environmental, and home-based testing interventions on the primary outcome, barriers related to AWD testing and secondary outcomes, as proportions stated in the objectives. The data collected from cluster sampling will be utilized to draw references and conclusion regarding possible causes of AWD amongst adults aged 15-49 years. In the research, random assignment of clusters shall be done among communities and not on the basis of individuals. This will prove to be advantageous by the fact that biases amongst intervention group and control group can be minimized. Moreover, credible and authentic results will be obtained that shall be easy to validate.
Choice of design
This study design has been chosen for the following reasons: it is best for evaluating either prevention/treatment or other specific interventions, it allows for research to be conducted with a reduced economy. The cost of interviewing every household or individual within the group would be very limiting. However, cluster sampling makes blinding more likely and minimizes the chances of selection and informed bias. Statistical analysis and validation of data are easily enabled using cluster sampling. This will be minimized by choosing a fair (unbiased) sample by way of simple random sampling of clusters. The sample will be large enough and a representation of the target population (adults 15-49 years).A Cluster sampling is a sampling method where populations are placed into separate groups. A random sample of these groups is then selected to represent a specific population. This is because the intervention in question (family practices that influence routine behaviour changes on AWD) directed to groups than individuals. Thus, the study requires cluster randomisation of geographical areas which will serve to minimise contamination risk (through exchange of information) between the interventions. This will involve interviewing study subjects 15-49 years in the affected communities of the five zones to complete at least 250 interviews (50 in each of the five zones) with members of the Somali communities. This will adopt semi-structured interviewing; participant observation and available published literature. Collection of data will be done with the assistance of local community based organization and active participation of local community leaders will be encouraged. In addition, sufficient training will be provided to data collectors reading tools and methodology to collect data. This will overcome any language barriers that might be faced during collection of data.
8.2. Sampling technique
A multi-stage random sampling technique will be used. The primary sampling unit (PSU) will be the sub-divisions. The sub-divisions will be enlisted and numbered 1-34. A simple computer-random generator (Stat Trek’s Random Number Generator) will be used to generate different random numbers. This will serve in the random selection of sub-divisions. In the second stage, 1 community per sub-division (PSU) will be randomly selected based on the generated random numbers to constitute the study area. The present sampling technique will help in identification of five communities that have similar population sizes and prevalence of AWD in such areas will be analysed. In addition, the natural characteristics and behavioural attributes amongst these communities will be taken into consideration. This will ensure that every attribute that related to prevalence and treatment interventions of AWD in selected communities are taken into consideration and accordingly data can be collected.
8.3. Data Collection
The method for data collection will be by use of structured interviews, questionnaires, telephone survey and examination of CTC and home records of the study participants. Data collection at baseline and home testing will be done by research assistants in a quiet, comfortable, private, and confidential area of the home. They will do repeated home visits before the intervention to create a relationship and gain the confidence of participants. Data collection tools will be developed according to National Norms and Standards for Cholera/AWD research adapted from WHO guidelines. Five research team members will be trained on data collection process and assigned in the five zones. Throughout the study duration, monitoring and evaluation data will be collected.
8.4. Data Analysis
Data collected will be analysed using the STATA statistical software for analytic/inferential statistics to estimate pattern and strength of associations among variables, test hypotheses. Descriptive statistics will summarize important features of numerical data. Data analysis and results reporting will be done according to the Extension of CONSORT statement to cluster trials that is; using the modified checklist to the standard CONSORT list. Data analysis will be done using the adjusted cluster-level intention- to- treat population to compare intervention and control arms at follow-up (3 months after implementation of the intervention). Continuous data will be expressed as mean, standard deviation if normally distributed or as median if not. For categorical data will be summarised as proportions.
Two stage analyses will be performed using cluster levels approaches. A summary measure of the proportion of Testing for AWD for each cluster will be estimated for the primary outcome using a Chi- square test. Random effect regression and generalised estimating equations approaches of binary outcomes (individual and cluster levels) with adjustment for covariates taken into consideration. The main covariates that will be considered for the research include age, gender, marital status, income, socioeconomic status and availability of health facilities. The analysis will be done with the STATA Software Package. All the obtained data will be used for intra cluster correlation. This will improve validity of results obtained from statistical calculations.
The clustering effect will be accounted for by the use of the chi-squared or F-tests both of which are divided by the design effect. Adjusted odds ratio (OR) and relative risk (RR) will be calculated at 95% confidence interval (for precision) as well as P-values for the different outcome variables. This data will further be interpreted and quantified.
9. Time schedule
|
Activity/Months |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
|
Protocol development and submission |
x |
x |
||||||||||||
|
Ethical clearance |
x |
|||||||||||||
|
Acquire funds/resources |
x |
x |
||||||||||||
|
Recruitment and training of project executors and data collectors |
x |
|||||||||||||
|
Designing and testing of Education materials, questionnaire, clinical forms |
x |
x |
||||||||||||
|
Recruitment of participants and baseline data collection |
x |
x |
x |
|||||||||||
|
Follow-up |
x |
x |
x |
x |
x |
x |
x |
x |
||||||
|
Data collection |
x |
x |
x |
x |
x |
x |
x |
x |
||||||
|
Evaluation of intervention implementation |
x |
x |
||||||||||||
|
Data entry and cleaning |
x |
x |
x |
x |
x |
x |
x |
x |
||||||
|
Data processing and analysis |
||||||||||||||
|
Report writing and Feedback |
||||||||||||||
|
Report Dissemination |
||||||||||||||
|
Publications |
10. Expected Output
The study intends to produce quarterly reports with a written thesis at the end of the study.
It is expected that current research will be published in a notable journal including Texila American University (TAU). The results of the study and the findings shall be presented across conferences within Africa and worldwide. The study will prove to be fruitful regarding outlining of current health complications within Africa and seek out various interventions in order to improve health status amongst citizens.
11. Societal and Scientific relevance
The social relevance in terms of family practices, risks, enablers and or behaviours will be highlighted strongly. The scientific aspects of the study will be categorised and its relevance to the society.
12. Ethical Considerations
The fact that this work will involve legal adult participants implies limited ethical issues but the due ethical requirement process will be followed including confidentiality rights. In any research I do, I am always keen to respect the perspectives of my participants and encourage open, and healthy discussion to make the research experience an enjoyable and meaningful one for all concerned; as such my research orientations are participatory ones, with a leaning towards focus group discussion, and interviews to encourage personal expression within a respectful social context. All information obtained from participants will be kept confidential by use of codes (initials not names) and their privacy highly ensured. Data collection tools and consent forms will be developed using national norms and standards for health research. I intend to provide feedback to key stakeholders during and after completion of the study. Data collection tools and consent forms will be developed using national norms and standards for health research. These will be pre-tested, reviewed, and validated by the research team. Co-investigators will train 5 of the research team members on data collection. Control clusters will receive information brochures about standard CTC care at baseline. After following and outcome analysis, evaluation will be done of the efficiency/benefits of the intervention and intervention offered to control arms if successful. Study results will be used to inform policy makers and to contribute to Cholera/AWD research literature
13. References (max. 1 page)
Aden, A.; Omar, M. and others (1997) ‘Excess female mortality in rural Somalia – Is inequality in the household a risk factor?’, Social Science and Medicine, 44.5: 709–15. Beauregard, R. (2017). Adapting Response Efforts to Stop the Spread of Acute WateryDiarrhoea. 4 May 2017. UNICEF Ethiopia. https://unicefethiopia.org/2017/05/04/adaptingresponse-efforts-to-stop-the-spread-of-acute-watery-diarrhoea/
Carruth, L. (2011) The aftermath of aid: Medical insecurity in the northern Somali Region of
Ethiopia. The University Of Arizona.
Crooks, A. T. and Hailegiorgis, A. B. (2014) ‘An agent-based modelling approach applied to
the spread of cholera’, Environmental Modelling and Software, 62: 164–77.
Food Security Analysis Unit. (2007). Somali Knowledge Attitude and Practices Study
(KAPS). Infant and Young Child Feeding and Health Seeking Practices. Nairobi: FSAU and
FAO.
Jentoft, Nina, and Torunn S Olsen. “Against The Flow In Data Collection: How Data Triangulation Combined With A ‘Slow’ Interview Technique Enriches Data.” Qualitative Social Work: Research and Practice (2017): 147-170. Web.
Maxwell, D. and Fitzpatrick, M. (2012). The 2011 Somalia famine: Context, causes, and
complications. Global Food Security, 1(1), 5-12.
Fisseha, B. (2016). Ethiopia – Response for Acute Watery Diarrhea outbreak in Moyale town.
WHO Ethiopia. http://www.afro.who.int/news/ethiopia-response-acute-watery-diarrhea-outbreakmoyale-town
Government of Ethiopia/OCHA (2017). Ethiopia: Humanitarian Response Situation Report No. 16 (November 2017). 30 November 2017.https://reliefweb.int/sites/reliefweb.int/files/resources/situation_report_no.16_november_2017_-
_final.pdf
Haileamlak, A. (2016). Why is the Acute Watery Diarrhea in Ethiopia Attaining Extended Course? Ethiopian Journal of Health Science, 26(5), 408.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5389054/
HIU (2017). Horn of Africa: Populations Impacted by Hunger and Disease (14 Sep 2017). US
Department of State- Humanitarian Information Unit.https://reliefweb.int/report/yemen/hornafrica-populations-impacted-hunger-and-disease-14-sep-2017
IFRC (2017). Emergency Plan of Action (EPoA) Somalia: Response to Acute WateryDiarrhoea (AWD)/Cholera Outbreaks. 24 April 2017. International Federation of Red Cross and RedCrescent Societies.https://reliefweb.int/sites/reliefweb.int/files/resources/MDRSO006Dref.pdf
Reaching nomadic pastoralists who are dispersed, highly mobile and at high risk of contracting AWD due to thelack of access to safe water and sanitation also need to be considered (Government of Ethiopia/OCHA, 2017: 9).
Kiros, B. (2016). Volunteers Blast Hygiene Message to Halt Acute Watery Diarrhea. 3
November 2016. UNICEF Ethiopia.https://unicefethiopia.org/2016/11/03/volunteers-blast-hygienemessage-to-halt-acute-watery-diarrhea/
Oxfam GB (2017). YEMEN: CATASTROPHIC CHOLERA CRISIS. Oxfam Briefing Note. 16
August 2017. ISBN 978-1-78748-036-0. Oxfam International.
https://www.oxfam.org/sites/www.oxfam.org/files/file_attachments/bn-yemen-cholera-160817-en.pdf
Peachey, Todd, Dianne J. Hall, and Casey Cegielski. “Knowledge Management And The Leading Information Systems Journals.” International Journal of Knowledge Management 1.3 (2005): 55-69. Web.
Lewis, Sarah. “Qualitative Inquiry And Research Design: Choosing Among Five Approaches.” Health Promotion Practice 16.4 (2015): 473-475. Web.
UNICEF (2017a). ETHIOPIA Humanitarian Situation Report #18 – Reporting Period 6 November– 5 December 2017.
https://reliefweb.int/sites/reliefweb.int/files/resources/UNICEF%20Ethiopia%20Humanitarian%20Situation%20Report%2018%20-%2005%20December%202017.pdf
UNICEF (2017b). UNICEF’s preventive plan to mitigate the risk of Acute Water Diarrhoea (AWD)and Cholera among Rohingya Refugees.
https://www.unicef.org/media/media_101029.html?p=printme
WHO (2017). Community engagement contributes to control of acute watery diarrhea in
Ethiopia’s Somali region. WHO Regional Office for Africa.
WHO Ethiopia (2017a). Looking out for Acute Watery Diarrhoea in Somali region: A day in thelife of a World Health Organization (WHO) surveillance officer in Ethiopia’s Somali region.http://www.afro.who.int/news/looking-out-acute-watery-diarrhoea-somali-region-day-life-world-healthorganization-who
WHO Ethiopia (2017b). WHO’s support to the response of the acute watery diarrhoea outbreakin Ethiopia’s Somali Region. July 2017. http://www.afro.who.int/news/whos-support-responseacute-watery-diarrhoea-outbreak-ethiopias-somali-region
Tull, K. (2017). Humanitarian interventions in Ethiopia responding to acute watery diarrhoea. K4D Helpdesk Report. Brighton, UK: Institute of Development Studies.
ANSWER
HEALTH SEEKING BEHAVIOUR WITH SPECIAL REFERENCE TO EPIDEMIC ACUTE WATERY DIARRHOEA (AWD) IN THE SOMALI REGION OF ETHIOPIA
Abstract
Acute Watery Diarrhoea (AWD) also known as cholera is a severe disease that is dangerous and life-threatening for the people of the Somali region of Ethiopia (WHO 2016). The continuous seasonal drought and/or flood in the region of Somali in Ethiopia caused the spread of the epidemic (UNICEF 2017). It not only affected the people of the region alone but has affected people throughout Ethiopia and the bordering countries (Kenya, South Sudan and Uganda).
The condition of the epidemic continues to be of great governmentconcern. The wellbeing of the people residing there is the main motive of the smooth-running of government. It has been identified that the cultural background and the unhygienic living practices of the people of Somali region are the major cause of the rapid spread of AWD diseases (UNICEF 2017). It has been considered that the education of the people is one of the solutions to the problem. However, the government of the Somali region of Ethiopia is working on the improvement of AWD detection machines and adopting measures to reduce the effects of the diseases. The conditions of such an epidemic affect the country’s economy and social structure. It has been observed in this dissertation research that the lack of awareness of the people of the Somali region, poor family hygiene practices, and inadequate medical facilities are the vital reasons for the outbreak of these severe diseases.
ACKNOWLEDGEMENTS
It provides me immense pleasure to present my dissertation, Health seeking behaviour with special reference to epidemic Acute Watery Diarrhoea (AWD) in the Somali Region of Ethiopia. This topic of research has helped me to gather immense knowledge about the disease as a public health concern, as well as the role of family hygiene practices and treatment seeking in the same.
I wish to extend my most sincere gratitude for those who have helped me to lead this research work towards a reality. Firstly, I thank those who have helped me to gather data throughout the research in the Somali region of Ethiopia. I would like to present heartiest thanks towards my direct supervisor and professor who have helped me to understand this topic and bring this study to a conclusion. I would also like to thank my colleagues, as well as friends who provided me with enough assistance to reach a definite goal. I acknowledge support of my family (Lilian, Dinah, Micheal, Isiah, and Malachi), and supervisors, as well as Professor Dr Shah Habib for his immense support in this study. Finally, I accept full responsibility for any limitations in this research.
Table of Contents
Abstract
ACKNOWLEDGEMENTS
CHAPTER
1. INTRODUCTION
Problem Statement
Background of Research
Research Aim
Research Objectives
Research Questions
Research Hypothesis
Rationale of the Research
Significance of Research
Dissertation Structure
Summary
2. REVIEW OF THE RELATED LITERATURE
Acute Watery Diarrhoea (AWD)/Cholera Situation
AWD Spread in the Regions (Kenya and Ethiopia)
Health System in Ethiopia (Somali Region)
Attitudes, Perception and Awareness amongPeople
Strategic Initiatives Taken by the Government
Role of Education in Preventing AWD
Search Strategy
PICO STATEMEN
Literature Searc
Inclusion and Exclusion Criteri
AWD Spread in the Region (Kenya and Ethiopia)
Health System in Ethiopia
Strategic Intervention Initiatives taken by the Government of Ethiopia and Implementing Partners
Awareness Among People
Role of Education in the Prevention of AWD Spread
Gaps in the Literature
Summary
3. RESEARCH METHODOLOGY AND DESIGN
Research Outline
Research Philosophy
Research Approach
Research Design
Choice of Design
Data Collection
Data Analysis
Limitations of Research Design
Research Method
Sampling Technique
Expected Output
Ethical Considerations
Validity and Reliability
Summary
4. DISCUSSION AND ANALYSES
Analysis of Quantitative Data
Summary
5. CONCLUSION AND RECMENDATIONS
Linking with Objectives
Recommendations
Limitations of the research
Future scope of the research
REFERENCES
CHAPTER
The repeated flood in the year 2006 was the main cause behind the situation of emergency disease outbreaks in the region of Somali in Ethiopia. The situation grew worse as around 76,081 cases of people suffering from severe watery diarrhoea were registered. The casualties of around 8,863 between the months of April and May 2007 brought fear to the minds of the native people. In August of 2017917 AWD cases were registered and 77,133 patients were suspected to be infected by cholera. Presently, the conditions of drought have forced the people to live in improper living conditions. It has been registered that around 766,000 people were forced to displace from their location due to severe drought in the region (WHO’S report on Somali, 2019). The recent mortality rate of the Somali region is 132/ 1000 live birth. Seeing the alarming situation, the government of Ethiopia requested the social agencies to come forward and help the people survive the situation of the epidemic. Social agencies like the Red Cross, WHO, UNICEF, and other partners came forward to help the needy and save the lives of people who were struggling with watery diarrhoea. The agencies provided clean utensils, treated water, and food for the people. They also provided bags consisting of ringer lactate. The severe condition of the people attracted the concern of the people worldwide. This dissertation is based on the health-seeking behaviours of the natives in the Somali region of Ethiopia suffering from acute watery diarrhoea epidemic.
Problem Statement
A wide knowledge-gap regarding family hygiene practices has led to the outbreak of Cholera/AWD in many sub-Saharan parts of Africa. The outbreak has been unpredicted and has spread up to the Somali region of Ethiopia and Moyale, a boarder point with Kenya. The situation remains unchanged even in the presence of various medical conditions. The main research questions of this dissertation are as follows:
-
What is the role of family hygiene practices regarding the spread of AWD/Cholera in the Somali region of Ethiopia?
-
What are the various factors that lead to the rampant transmission of AWD among adults aged 15-49 in the Somali region of Ethiopia?
-
What are the various behavioural, social, and cultural attributes within this region that aids in prevention and treatment of AWD/Cholera?
-
What measures need to be undertaken for the reduction in the spread of the AWD in the Somali region?
-
What are the recommendations regarding interventions implemented by Government, Non-Governmental Organisation (NGOs), and stakeholders for the treatment and prevention of AWD/Cholera?
Background of Research
This dissertation’s primary focus was on the behaviour of the Somali natives in the Somali region of Ethiopia and their reaction towards the epidemic. The study sought to identify the outlook of the people, their knowledge, and family hygiene practices upon the occurrence and spread of the diseases. The study also aimed to educate people about the consequences of acute watery diarrhoea and its effects on human health. Further this dissertation study sought to explain the role of the native people, their hygiene practices, and the medical facilities available for the curing process if these diseases occur.
Research Aim
The research aimed to identify the family hygiene practices of the people residing in the Somali region of Ethiopia in preventing the epidemic of AWD within the first 90 days of infection.
Research Objectives
The following objectives were selected for the proper study of the topic:
-
To evaluate the healthy practices adapted by citizens of Ethiopia from the Somali region regarding Acute Watery Diarrhoea (AWD).
-
To identify the extent of awareness, attitude shaping, and treatment seeking about AWD among the Somali region people.
-
To identify the factors that has impacted the health seeking behaviours of the Ethiopia region people.
-
To provide recommendations of strategies that will assist the Somali region of Ethiopia people to upgrade their health-seeking behaviours.
Research Questions
The research question which framed this study is as follows:
-
What are the health seeking behaviours of Ethiopia citizens from the Somali region regarding Acute Watery Diarrhoea?
2 To what extent are the people of the Somali region aware of Acute Watery Diarrhoea?
3. What factors have impacted the health seeking behaviour of the Ethiopia region people?
4. What strategies can be adopted by Somali region people to upgrade their health-seeking behaviours?
Research Hypothesis
H0= Health seeking behaviour of people residing in Somali region have a strong positive significant correlation with increased intensity of AWD.
H1= Health seeking behaviour of people residing in Somali region have no significant correlation with increased intensity of AWD.
Rationale of the Research
AWD is a severe disease that is dangerous and life-threatening. Theoutbreaks in the Somali region of Ethiopia are often cyclical and man-made causing substantial morbidity and mortality (Unicef.org, 2016). While there are some contextual and environmental factors involved, such as decreased rainfall and decreased vegetation cover, the conflict and poor family hygiene practices are the main contributing factors to the outbreaks (Unicef.org, 2016). This becomes complex with limited water access, latrine use, and poor food handling practices for AWD prevention and treatment seeking. Outbreaks of diarrheal disease, including AWD/cholera, further worsen the situation of ongoing drought and conflict (US Department of State Humanitarian Information Unit. This can occur as a short outbreak or as a protracted epidemic. The transmission of the causative bacteria is through the faecal-oral route of contaminated food and/or water caused by poor sanitation practices (Unicef.org, 2017) It not only affected the people residing in the region, but these outbreaks also affected people of the entire region of Ethiopia in some manner.
The government is concern about the health condition of their people the smooth running of the government is only possible with the social wellbeing of the people residing there. The economy as well as the social condition of the country is dependent on the heath condition of the people.
The real issue is not the rain as the region is mostly drought- prone. The important aspect of the precipitation is the failure of seasonal rainfall for the third consecutive year across the country. This has resulted in crop and livestock losses, associated food insecurity, acute malnutrition, and greatly diminished water resources including dried up wells, with seasonal rivers and streams drying up (Unicef.org, 2017).
Increased malnutrition has made communities vulnerable to communicable diseases, for example, cases of malnutrition with AWD have been reported in women and children, which require special care. In areas experiencing acute malnutrition, outbreaks of measles are also likely to occur. Limited access to water has forced people to use water that is not always safe. This puts them at risk of AWD and other diarrheal diseases.
The condition is still an issue as the consequences are severe and the measurement is not yet proper. The awareness of the people is very important for the prevention and management of these diseases. This epidemic condition of the Somali region of Ethiopia is appropriate for a research topic as it shows the effects of the life-threatening epidemic and the need to identify proper measures which requires close analysis to be cured.
Significance of Research
The research is very significant in the proper analysis of the local citizens of the Somali region of Ethiopia and their role in the prevention of the AWD within the first 90 days of their intervention. The information and the data analysis done in the research study shall be beneficial for the future research purposes and will serve as a good source of literature for future generations.
Dissertation Structure
The first chapter consists of the introduction which includes the research objectives and purpose, as well as the guiding research questions which frame the study. The second chapter includes the analysis of the relevant professional literature. The third chapter of this research paper highlights the methodologies of quantitative and qualitative data analyses. Methods of data collection are presented and provide effective information regarding the dissertation topic. The fourth chapter addresses the proper analyses of the collected data. Finally, the fifth chapter consists of the recommendations and conclusion of the research study.
Summary
This dissertation research is vital to aide in promoting the proper understanding of the people regarding the consequences of the Acute Watery Diarrhoea. The research included a close analysis of the behaviour of the people and may serve to help them by making them more of the many aspects regarding these diseases (Azage & Haile, 2015). The study also helped in analysing the different family hygiene practices and medical facilities, as well as the social agencies for providing medical interventions to people affected in the active zones.
The proper analysis of the different literature reviewed is vital for the understanding of the point of view of the different writers on the related topics. The watery diarrhoea is common in areas with poor sanitation conditions and poor family hygiene practices. The repeated flood in the Somali region of Ethiopia in the year 2006 increased an unhealthy condition in their region which was the main cause of the severe diseases. Somali, being a drought prone area, has made the living condition of the people very difficult. It has been reported by the WHO (2017), which around 766,000 people was forced to leave their homes and move to safer regions to survive in better living conditions. The proper study of the existing literature supports the importance of the research topic and derives the research questions. The report of UNECEF and WHO has provided relevant information about the epidemic condition of Somali region (Unicef.org, 2017). The gaps in the different literature reviews were helpful in the identification of the research problems for further study. The statistics provided in the annual report clarifies the intensity of the epidemic in the area.
Acute Watery Diarrhoea (AWD)/Cholera Situation
Drought, famine and cholera/AWD (Acute Watery Diarrhea) outbreaks have become recurrent in the Horn of Africa (WHO, 2017).The Somali region of Ethiopia is no exception. Drought naturally contributes to trigger increases in epidemics such as AWD and measles, some of which are cross-border outbreaks (Unicef.org, 2017). AWD remains a significant public health problem in many parts of the Somali region of Ethiopia, where the disease can spread quickly unless an outbreak is stopped. This underpins the international partners evidence on humanitarian responses to AWD in Ethiopia, in terms of necessary cross district and/or cross border co-ordination, as well as the human and financial resources needed assessed their own AWD responses in Ethiopia and neighboring countries. In developing countries, up to 50 percent of cases die from dehydration and kidney failure if not adequately rehydrated. Infection without symptoms or with only mild diarrhea also occurs, particularly in children (Unicef.org, 2016).
AWD diseases are contagious waterborne diseases that are transmitted through Vibrios cholera. The disease is highly contagious and is transmitted mainly through unsafe drinking water and often by undercooked seafood (WHO, 2016). Symptoms may appear as soon as within a few hours or after five days. The main symptoms include large volumes of fluid loss through watery diarrhoea, often termed as ‘rice water stools’, vomiting, leg cramps, circulatory collapse, and shock. Fatality occurs in 25-50% of the cases in absence of proper treatment (Cdc.gov, 2016).It kills within short time if patients are not rehydrated and given adequate mineral and liquid balance needed in human body. The risk increases at epidemic proportions in regions with poor water, inadequate sanitation facilities, lack of health facilities, poverty-stricken areas, overcrowding, drought, conflicts, insecurity, and uncontrolled areas of water sources (Hazel, Elizabeth, Jennifer Bryce, and IIP-JHU iCCM 2016).
In 2016, WHO and its partners, acknowledged the continued public health threat posed by the disease; the enduring problems of lack of access to clean water, inadequate sanitation; and the absence of any long-term impact on cholera incidence through perennial responses to major outbreaks. Mass urbanization, climate change, and growing competition for water resources may, in fact, contribute to further increases in the AWD burden (WHO, 2016).
AWD Spread in the Regions (Kenya and Ethiopia)
From late 2014 to the end of 2015, AWD outbreak has seized 30 of the 47 counties of Kenya causing close to 7,000 cases of morbidity and over 100 deaths. The outbreak occurred in part due to the El Niño floods which created favorable conditions for the spread of the causative bacteria. After spreading in Kenya for over a year, the disease moved to Ethiopia (Memirie, 2016).
In Ethiopia, AWD was first reported in districts of Oromia and Ethiopian Somali close to the Ethio-Kenyan border (Moyale) in February of 2016. Thereafter, it continued spreading east and north reaching many parts of the country including the capital city, the northern parts of the country, and the Somali region of Ethiopia remain the hardest hit due to several factors (Memirie, 2016). One of the major factors despite an ongoing effort to contain the outbreak, it continued spreading to large areas of the country affecting many people; its course remained protracted and kept many people at risk.
The Cholera/AWD risks factors that propagated the spread of the disease are:
-
Water, Sanitation and family hygiene practices: Insufficient water access, population density, poor awareness about the disease, and way of life. Violence prevents people from accessing adequate water sources, displaces them to settlements with poor water and sanitation, and hinders them reaching health care centres. In addition, in a drought, water becomes scarce and pathogens accumulate in stagnant waters, and people and cattle are pushed to use these contaminated waters thus sharply increasing the risk of a cholera/AWD epidemic (Eshete, Abebe, & Gudina, 2015).
-
Demographic and social factors: Demographic explosion especially in big cities-associated with poverty and disordered urbanization is a key factor in the occurrence of the outbreak. Big gatherings (pilgrimages and celebrations), communal eating practices that favour overcrowding and lack of hygiene practices at family level are risk factors that exacerbate outbreaks (Eshete, Abebe, & Gudina, 2015).
-
Climatic condition (Famine, drought): AWD outbreak is known to occur in humid and inter-tropical zones during rainy seasons. Flooding during rainy seasons can support the emergence or the upsurge of AWD outbreak. Although the causative bacteria are more delicate in the atmospheric environment than in its aquatic environment, it can survive well for days on fruits and vegetables. Ecosystem changes due to global warming, environmental pollution, drought, deforestation leading to floods, and other climatic disasters are the reason for the upsurge of AWD outbreak (Eshete, Abebe, & Gudina, 2015).
Health System in Ethiopia (Somali Region)
The health system of the Somali region of Ethiopia is very poor the people are suffering severely with numerous diseases. The diseases are mainly the reason for the poor health condition of the Somali natives. The low economic condition of the people and the poor medical facilities available are the main cause behind the outbreak of diseases like watery diarrhoea (Berhe, Abadi, & Yitayih, 2014).The people residing in the Somali region are mainly in the lower economic section of Ethiopia (Dagnew et al.2012). The food intake is not healthy and thus they are unable to support their immune systems from numerous diseases. The poor sanitation conditions are among the vital reasons for the outbreak of the epidemic diseases (Beyene & Hunachew, 2018)
The acute watery diarrhoea is caused by the impure or unsafe water. The repetitive flooding in the region of Somali in Ethiopia was at times the main reason behind the occurrence of the epidemic diseases. The unavailability of the proper medical facilities in the region causes a huge amount casualty (Degebasa, 2017). The conditions became so unbearable that the government of Ethiopia was bound to request the social agencies to come forward and help the people suffering from the severe situation (Eshete, Abebe, & Gudina, 2015).
The proper availability of medical facilities is very important for the country to manage the severe epidemic. The lack of proper medical facilities in Somali was the main reason behind the severe epidemic which resulted in the loss of numerous people. The government of Ethiopia is working towards increasing the literacy rate of the citizens (UNICEF, 2017). The collaboration of the government with UNESCO has enabled the children, as well as the adults to increase their knowledge concerning AWD. Schools have established in the rural areas, such as the ABE School, which motivated the children to take- up a healthy lifestyle. Hence, it is observed that statistics of the people reported to be affected by the diseases was alarming (Getachew et al. 2016).
Attitudes, Perception and Awareness among People
The people of the Somali region of Ethiopia do have several challenges such as illiteracy, poor infrastructure, and medical facilities and are unaware of the causes of AWD spread and prevention. The awareness of the people is very important. The prevention of the epidemic is possible with proper awareness and prevention interventions. The government must take up the initiatives of supporting the people and imparting proper knowledge about the consequences of life-threatening epidemic diseases (Mohammed et al. 2016). The people needed to be aware of the importance of proper sanitation. The clean environment around the residence helps them to stay free of diseases. The proper maintenance of their surroundings is very important for the people of the Somali region of Ethiopia (Teferi, 2015). The natives need to be educated properly about the causes and consequences of the diseases. It is very important for the government of Ethiopia to adopt different awareness campaigns to make people aware and prevent the diseases like AWD (Eshete, Abebe and Gudina, 2015) The role of the key stakeholders, partners, and NGOs is also recommendable in supporting relief from the conditions of a severe epidemic. The non-governing agencies take up much initiative and organize various programs to make the people aware of the consequences and effects of the diseases (Warsame, 2016). The people residing in Somali region of Ethiopia also need to have a clear idea about the positive side of living a civic life. The citizens need to take care of the self-sanitation and strive to keep their surroundings clean. This will help the citizens to live a healthy life (Woldie, Yigzaw, & Amare, 2015).
Strategic Initiatives Taken by the Government
The Somali region of Ethiopia has very poor medical conditions. The government must take up the initiative to improve the healthcare facilities. The presence of just 10 hospitals in the area makes it very difficult for the people of the Somali region to obtain proper medical facilities (Shaw, et al. 2015). The entire region has just one research lab which is not enough for the entire population of Somali. The mobile and nutrient team work efficiently to provide relief to the people residing in the area (Tefera, 2015). The government facilities regarding the healthcare are not adequate in the Somali region of Ethiopia. It is very difficult for the same number of hospitals to accommodate and cure such a large population. The government of Ethiopia was forced to seek help from the agencies such as; Somali Regional Bureau for Health, development partners, UN family, and Red Crossto help the people in preventing the epidemic.
Role of Education in Preventing AWD
Awareness and education are the two most important criteria for the prevention of the epidemic diseases. The proper education among the masses of Somali region of Ethiopia will help the citizen to understand the condition better and adapt interventions that shall prevent the consequences of the AWD (Tuem et al.2018).The government and the non-governmental agencies must take up initiatives to educate the people and make them aware of the consequences and effects of the diseases (Gebremedhin et al. 2016).
The programmes arranged by different agencies from time to time help the people of the Somali region of Ethiopia to understand the importance of living a healthy life. The people are taught to live life in proper healthy conditions. It is vital for the people to take sanitation into consideration. The people are educated to use modern ways in their day to day activities to make their surroundings clean and a better place to live in (Tefera, 2015).
Search Strategy
Keywords improve specificity and credibility of research being conducted Venkatesh, Brown & Bala, 2015). Various keywords used for obtaining relevant literatures in accordance to the topic are below. Some of the keywords included: Cholera/AWD outbreak; AWD testing and counselling, family practices, behaviours, adults, and Somali region of Ethiopia. The MESH terms used for research include; AWD, diagnosis, prevention, adults (Gizawet al. 2018). Various databases were searched for obtaining appropriate literature. Some of the databases included Google Scholar, Pub Med, and Pub Med Central. Boolean search strategy was used using AND/ OR as outlined below:
|
KEYWORDS |
AND/OR |
KEYWORDS |
AND/OR |
KEYWORDS |
|
AWD* |
AND |
AWD testing |
OR |
AWD family practices * |
|
AWD family practices* |
OR |
AWD behaviours |
OR |
AWD diagnosis* |
|
AWD diagnosis |
AND |
AWD Counselling |
AND |
Adults |
|
AWD Counselling* |
AND |
Adults |
AND |
Somali region of Ethiopia |
|
AWD testing |
OR |
AWD diagnosis* |
AND |
AWD family practices |
Table 1: BOOLEAN Search Strategy was used
Note, (Gebremedhin, Mamo, Gezahign, Kung’u, & Adish, 2016, pp.457-459)
PICO STATEMENT
PICO STATEMENT
Table 2: PICO Statement
(Note.Gebremedhin, Mamo, Gezahign, Kung’u & Adish, 2016, pp.457-459)
Literature Search
Several suitable peer reviewed qualitative and qualitative studies regarding AWD prevention and treatment for 15-49 years adults’ were analyzed. Moreover, studies reporting AWD prevalence in Somali region and the whole of Ethiopia, East Africa, Sub-Saharan Africa, and Asia were collected from several databases such as PubMed, PubMed Central, and Global Health. Articles that were published after 1970, that is after the break-out of the disease were also studied. Furthermore, additional studies were sorted from both the references and related citation lists next to the Pub Med summary list (Birhanu, Abadi & Shimels Ayalew, 2018, pp. 194-202). Official WHO, CDC, UNICEF, UNHCR, UHI, UNAIDS sites, and National Government Agency sites, as well as reports were thoroughly searched. However, one of the national reports included was in Ethiopia due to its high relevance. Additionally, 2,640 peer-reviewed articles and reports were identified and further screened.
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria were used for analyses of relevant data. Setting-up of exclusion and inclusion criteria added to the specialist of research and ensured progress of data in a definite direction (Memirie, 2016). The search process was narrowed down and journals with irrelevant data were excluded. The inclusion and exclusion criteria were enlisted as shown in following table:
|
Inclusion Criteria |
Exclusion criteria |
|
● Target population (adults 15-49 years) ●Presence of proper experimental methodology ● Presence of systematic review of literatures within journals with evidences ● Availability of statistical data ● Authentic and peer reviewed journals ● Evaluation of data at 12 months |
●Individuals younger than 15 years and older than 49 years ● Lack of literature review and evidences ● Lack of credible sources regarding data within journals ● Lack of statistical information ● Non-peer reviewed journals ● Evaluation of data beyond 12 months |
Table 3: Inclusion and Exclusion Criteria
(Note. Influenced byWamai & Richard 2014, pp.75-95)
Figure 1: Conceptual framework

(Note. Influenced byLewis, 2018, pp.473-475)
Gaps in the Literature
There are several literatures regarding identification of interventions regarding AWD health seeking behaviours (testing and treatment) seeking strategies. In the present context there exists a profound lack of knowledge regarding family hygiene practices that promote health seeking behaviours in the first ninety days of AWD interventions.
Moreover, most of the studies were conducted in Asia, USA, and Haiti where the prevalence of disease is completely different from that of Somali region of Ethiopia (Singh etal, 2016). The current research focuses on promotion of awareness on health seeking strategies and does not confine itself to coping and behavioural risk reduction programmes. In addition, there exists a gap in knowledge regarding nutritional services and clinical trials conducted for finding treatment protocols of AWD/Cholera. There is a need for research focused on the prevalence and intervention methods specified towards the Somali region of Ethiopia to promote better health seeking behaviours among people. The proper identification of the intervention by effective monitoring is useful at this stage.
Some studies presented in media newsletters and blogs are excluded because of limited credibility of source and a lack of approaches that led to promoting good family hygiene practices or health care seeking for AWD services. In general, most gaps that were identified with the studies were that they did not discuss further intervention strategies but rather mentioned them broadly. Most of the studies/reviews conducted were outside the Somali region of Ethiopia, a gap that indicated a limited study of AWD on health care seeking behaviors (family practices) in this setting (Yilmaet al. 2016).With this background, there is need for more studies to assess the role played by family hygiene practices in promoting health seeking behavior with special reference to epidemic Acute Watery Diarrhea (AWD) in the Somali region of Ethiopia in the first ninety days of AWD intervention.
Summary
The broad study of the proper literature review provides an overall idea about the research topic. This also identified areas in need of further research and served to develop the framework of the research problems to be addressed. Further, the literature review was helpful in the proper execution of the research study. The study was conducted on the correct path due to the defined proper study methodology, well designed instruments, and a thorough review of relevant literature pertaining to the topic of this dissertation.
Within this research study a triangulation approach was applied. Both qualitative and qualitative approaches were used. However, a substantial amount of information was collected through qualitative analysis of articles. The process allowed the research to be flexible in nature while maintaining its specificity towards fulfilment of its objectives (Shaw & Brya, 2015). The data regarding the prevalence of data was collected from adults belonging to age group 14-49 years of age. In addition, five areas (Zones) were used for collecting data namely; Jigjiga, Jarar, Dollo, Shabelle and Fafan of the Somali region in Ethiopia. The sampling technique for research subjects was random sampling selected from the affected zones. The data analysis was done using correlation analysis technique. The collected data was primary and secondary data. The data was collected using questionnaires, interviews, observations, and set reading of published research material including both present and historical information on disease outbreaks, mainly Acute Watery Diarrhoea (AWD) sometimes known as Cholera (Desai et al. 2015).
Research Outline
|
Research outline |
|
|
Research approach |
Deductive |
|
Research Philosophy |
Positivism |
|
Design of the Research |
Descriptive |
|
Research methodology |
Quantitative and qualitative |
|
Method for data collection |
Primary |
Table 4: Research Outline
(Note.Influenced by Bell etal.pp.255-260)
Research Philosophy
The positivist philosophy of research was the selected form of the different philosophical approaches of research like that of positivism, realism, and interpretive. The use of positivism is helpful in analysing the data in an organised manner (Bell et al., 2018, pp. 255-260). The philosophy was essential in the execution of the qualitative data. The proper analysis of the collected information was possible with the help of data and statistical representation (Shaw, Bryan, et al., pp.636-647).
The collection of the first-hand data was possible with the help of the positivist philosophy. The interpretive were the philosophical approaches that mainly used the past literature relevance’s for reaching to the conclusion of the selected research studies, on the other hand, the realism sought to identify the current perception of the various people under study regarding the currently selected topic (Sekaran & Roger, 2016, pp. 25-35). Both interpretive and realism philosophic were not considered in the selected research study hence the positivism was used.

Figure 2: Types of philosophy
(Note: From Ponterotto, 2013, p.46)
Research Approach
The two main approaches of the research studies were the inductive and the deductive approaches. The inductive approaches tend to create a new theory. On the other hand, the deductive approaches seek to test the previous test on the specific topic of study and try to find the change in the aspect with time. The scenarios do not remain same all the time and keep on changing (Wamai, 2014). This research approach selected in this dissertation was the deductive approach. As there was much research done previously on a similar topic and hence it was important for the research study to identify the changes in the scenario and the current situation of the native Somali people in the Somali region of Ethiopia.

Figure 3: Types of research approach
Note: Influenced by views of Creswell, 2013, p.61)
Research Design
A cluster sampling was designed (qualitative, quantitative, comparative, and analytical in nature) to assess the role played by family practices in promoting health seeking behaviors that shape prevention and treatment seeking using a combination of health education strategies (intervention) on AWD testing and sustaining good family hygiene practices among adults aged 15-49 years in five communities. This was compared to standard care seeking (control) in five communities of the Somali region of Ethiopia. The study involved evaluating the outcome of a combination of biomedical, behavioral, environmental, and home-based testing interventions on the primary outcome, barriers related to AWD testing and secondary outcomes, as proportions stated in the objectives (Alemayehu et al. 2018). The data collected from cluster sampling was utilized to draw references and conclusions regarding possible causes of AWD amongst adults aged 15-49 years. In the research, random assignment of clusters was applied among communities and not based on individuals. This proved to be advantageous by the fact that biases amongst intervention group and control group could be minimized. Moreover, credible and authentic results were obtained that were easy to validate.

Figure 4: Types of research design
(Note. From Yin, 2013, p.33)
Choice of Design
This study design was chosen for the following reasons: it was best for evaluating either prevention/treatment or other specific interventions, and it allowed for research to be conducted with a reduced economy. The cost of interviewing every household or individual within the group would have been very limiting (Memirie, 2016). However, cluster sampling made blinding more likely and minimized the chances of selection and informed bias. Statistical analysis and validation of data were easily enabled using cluster sampling. This was minimized by choosing a fair (unbiased) sample by way of simple random sampling of clusters.
The sample was large enough and a representation of the target population (adults 15-49 years). A cluster sampling is a sampling method where populations are placed into separate groups. A random sample of these groups was then selected to represent a specific population. This was because the intervention in question (family hygiene practices that influence routine behavior changes on AWD) directed to groups more than individuals. Thus, the study required cluster randomization of geographical areas which served to minimize contamination risk (through exchange of information) between the interventions. This involved interviewing study subjects 15-49 years in the affected communities of the five zones and completed at least 250 interviews (50 in each of the five zones) with members of the Somali communities. This adopted semi-structured interviewing; participant observation, and available published literature. Collection of data was done with the assistance of local community-based organizations and active participation of local community leaders was encouraged. In addition, enough training was provided to data collectors reading tools and methodology to collect data. This overcame any language barriers that might be faced during collection of data as each tribal group surveyed has their own dialect which is difficult to understand.
Data Collection
The method for data collection was structured interviews, questionnaires, telephone survey and examination of CTC and home records of the study participants. Data was collected at baseline and home testing was done by research assistants in a quiet, comfortable, private, and confidential area of the home. They repeated home visits before the intervention to create a relationship and gain the confidence of participants. Data collection tools were developed according to National Norms and Standards for Cholera/AWD research were adapted from WHO guidelines. Five research team members were trained on data collection processes by conducting mock interview session and assigned in the five zones with proper briefing about the data collections methods. Throughout the study duration, monitoring and evaluation data were collected.
Data Analysis
Data collected was analyzed using the STATA statistical software for analytic/inferential statistics to estimate pattern and strength of association’s among variables, test hypotheses. STATA is the most commonly used statistical software used in the research work for data analysis. Descriptive statistics summarized important features of numerical data. Data analysis and results reporting were done according to the Extension of CONSORT statement to cluster trials that was applied with the modified checklist to the standard CONSORT list. Data analysis was done using the adjusted cluster-level intention- to- treat population to compare intervention and control arms at follow-up (3 months after implementation of the intervention). Continuous data were expressed as mean, standard deviation if normally distributed or as median if not. Categorical data was summarized as proportions.
Two stage analyses were performed using cluster levels approaches. A summary measure of the proportion of testing for AWD for each cluster was estimated for the primary outcome using a Chi-square test. Random effects regression and generalised estimating equations approaches of binary outcomes (individual and cluster levels) were made with adjustments for covariates taken into consideration. The main covariates that were considered for the research included age, gender, marital status, income, socioeconomic status, and availability of health facilities. The analysis was done with the STATA Software Package.All the obtained data were used for intra cluster correlation. This improved the validity of results obtained from the statistical calculations. The clustering effects were accounted for using the chi-squared or F-tests both of which were divided by the design effect. Adjusted odds ratio (OR) and relative risk (RR) were calculated at 95% confidence interval (for precision) as well as P-values for the different outcome variables. This data was further interpreted and quantified.
Limitations of Research Design
The research faced several limitations. The time was the major issue faced while conducting the research. The collection of primary data was very vital and needed proper time to collect proper data by interviewing the people belonging to the different communities. The language was a huge barrier (Cronin et al. 2016). The people belonging to different communities had a different language. This made it very difficult for the researcher to convey their questions properly to the participant when they conducted an interview (Venkatesh, 2014). The resource was also a big challenge for the researcher. The unavailability of proper resources restricted the researcher from conducting the proper execution of the research approaches. The sampling of the data was also a great problem. The collection of the authentic data and sampling it properly needed to be done in a much-organised manner (Bryman & Bell, 2013). The data collected by the interview was used for the statistical analysis and hence needed to be correct to solve the research problems.
Research Method
Qualitative, as well as quantitative methods were selected for the execution of the research study. Both methods had their own importance in the study. The quantitative methods were used for the proper analysis of the statistical data representation (Venkatesh, et al, 2015). The proper numerical representation of the statistical analysis was possible with the help of the quantitative data. The quantitative data were very helpful in the further understanding of the statistical data. On the other hand, the qualitative data was used for the non-measurable units like that of emotions and feeling. The proper analysis of the feeling of the people was very important. It was needed to take the emotion of the people of Somali into consideration to have a correct approach towards the research problems. The qualitative data, as well as the quantitative data, were beneficial for the research study.
Sampling Technique
A multi-stage random sampling technique was used. The primary sampling unit (PSU) was the sub-divisions. The sub-divisions were enlisted and numbered 1-34. A simple computer-random generator (Stat Trek’s Random Number Generator) was used to generate different random numbers. This served in the random selection of sub-divisions.
The occurrence of biases outcome was avoided with the help of the multistage random sampling. In the second stage, 1 community per sub-division (PSU) was randomly selected based on the generated random numbers to constitute the study area. The present sampling technique helped in identification of five communities that had similar population sizes and prevalence of AWD in such areas was analysed. In addition, the natural characteristics and behavioural attributes amongst these communities were taken into consideration. This ensured that every attribute that related to prevalence and treatment interventions of AWD in selected communities was taken into consideration and accordingly data was collected.
Expected Output
The study intended to produce quarterly reports with a written thesis at the end of the study.It was expected that current research would be published in a notable journal such as Texila American University (TAU). The results of the study and the findings were presented across conferences within Africa and worldwide. The study proved to be fruitful regarding outlining of current health complications within Africa and sought out various interventions to improve health status amongst citizens in the study area and beyond.
Societal and Scientific Relevance
The social relevance in terms of family hygiene practices, risks, enablers, and/ or behaviors were highlighted strongly. The scientific aspects of the study were categorized and its relevance to the society was noted.
Ethical Considerations
It was important for the researcher to maintain certain ethical considerations in the proper execution of the research approaches. The ethics were very vital while collecting information. The researcher needed to be very specific and clear with the questions asked. The nature of the person being interviewed was also very important (Sekaran & Roger, 2016, pp. 25 -35).
The fact that this work involved legal adult participants implied limited ethical issues, but the due ethical requirement process was followed which included confidentiality rights. In any research I’ve done, I am always keen to respect the perspectives of my participants and encourage open, and healthy discussion to make the research experience an enjoyable and meaningful one for all concerned; as such my research orientations are participatory ones, with a leaning towards focus group discussion, and interviews to encourage personal expression within a respectful social context. All information obtained from participants was kept confidential by use of codes (initials not names) and their privacy highly ensured. Data collection tools and consent forms were developed using national norms and standards for health research. I intended to provide feedback to key stakeholders during and after completion of the study.
Data collection tools and consent forms were developed using national norms and standards for health research. These were pre-tested, reviewed, and validated by the research team. Co-investigators were trained and there were five research team members who collected data. Control clusters received information brochures about standard CTC care at baseline. After following and outcome analysis, evaluation was done of the efficiency/benefits of the intervention and intervention offered to control arms if successful. Study results may be utilized to inform policy makers and to contribute to Cholera/AWD research literature.
Informed Consent
The proper execution of the data was very important. It was important that the researchers maintained the law and order of the place and did not adopt any inconvenience of means for the execution of their research studies (Bell et al., 2018, pp. 255-260). The maintenance of transparency was very vital for the proper and effective execution of the research problems.
Respect to Privacy
It was important for the researcher to maintain the privacy of the person they were participant interviewed. There might have been as it auction where the person was not willing to provide personal details. The privacy of the person needed to be respected by the researcher, and it was important for them to let the interviewer maintain his own privacy as well. The researcher made a conscious effort to not make the interviewee uncomfortable while collecting information from them.
Protection of Collected Data
The researcher made sure that the data they were collecting from the personal interviews was kept properly. This information was personal and needed to be handled with care. The researcher ensured that they did not disclose the data in any concern. The maintenance of the collected data was the huge responsibility of the researcher.
Maintaining Genuineness of the Data
The researcher needed to be very specific about the genuineness of the data used in the research. As the data used for the research purpose was primary in nature and were collected by the personal interviews, hence it was vital to have provided the genuineness of the research work (Wamai, 2014, pp. 75-95).
Validity and Reliability
The research topic was valid and was based on the realness as a dimension. An area of Somali located in Ethiopia was considered for the research study. The people of five different communities with almost equal population were selected for the interview. The people from each community were interviewed for the research (Wamai, 2014, pp. 75-95). The purpose of selecting this area was the huge number of reported people who were suffering from the AWD. The epidemic outbreak of the area was the prime reason for the selection of this research topic. This topic was valid and had a real implication.
Summary
The use of methodological approaches was necessary for the proper execution of the research problems. The proper selection of the philosophy which was positivism for the present study needed to be very specific as it had the potential to have changed the entire perspective of the research topic. It was very important for the researcher to make sure that they could overcome the challenges in the effective execution of the research.
The proper analysis of the various collected data is needed for the effective understanding of the behaviour of the people residing in the Somali region of Ethiopia. The collection of data was done with the help of primary data collection using a questionnaire and survey schedule. The data was collected from the five different communities of the Somali region with almost the same population sample. The analysis was helpful in the better understanding of the attitude and family hygiene practices of the people towards the epidemic of AWD.
Analysis of Quantitative Data
The collected quantitative data sets were used in the analyses of the different demographic factors of the respondents as well as the factors related to the family hygiene practices. The statistical representation of the collected data enabled the clear understanding of the current scenario of the Somali region. This helped the government of Ethiopia to identify the correct strategies to overcome the situation of epidemic of AWD in the Somali region of Ethiopia.

Figure 5: Gender of respondents
A total of 732 people were surveyed for collecting data. There were 632 female respondents whereas only 100 respondents were male. The main reason for most female respondents was that most of the males were out for work during the time of data collection. It was the female respondents who were in their home and provided the necessary data during the survey.

Figure 6: Education level of respondents
The area was deprived of proper formal education. Out of 698 respondents, it was analysed that 542 of the respondents or 72.8% were lacking any formal education; 12.1% of the respondents only had a primary level of education; and just 1.3% was able to obtain tertiary education. The level of education showed the reason for the vulnerable situation of this area.
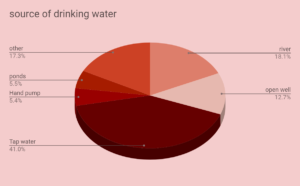
Figure 7: Source of drinking water
The analysis of survey data revealed: 18.1% of the respondent used river water for consumption; 12.7% of them relied on the open well; 41% of them used water from the tap; and around 5.5% of the respondents used water from hand pump and ponds. The use of unhygienic water was the main cause behind the outbreak of the AWD. The lack of knowledge and the inability of the proper drinking water were the reasons behind such use.
Attitude: If respondents consider their water to be safe for consumption

Figure 8: Attitude: If respondents consider their water to be safe for consumption
The lack of proper knowledge indicated the respondents were uninformed about hygiene and sanitation practice levels. Around 89.4% of the people believed that they were using safe drinking water and there was no harm in doing so. Survey results showed 6.9% of the respondents admitted that the water that they were using was not safe for consumption.

Figure 9: If respondents treat the water before using it for drinking or another purpose
It was noted that around 75.8% of the respondents admitted that they treat their water before drinking while 23.8% of the respondents did not believe in treating the water before consuming it. This data indicated that there was a lack of proper knowledge which was the major reason for the uninformed behaviour of the people concerning their safety towards health.

Figure 10: What respondents use to treat water
Around 64.9% of the respondents said that they use chemicals for making their water was fit for consumption. While 7.4% of the respondents stated that they boiled the water before drinking. Only 1.75% of the respondents used another source for the purification of the water.

Figure 11: If they often wash their hands
The respondent during the data collection admitted that around 89% of them have the tendency of washing their hands frequently while around 7.8% denied the fact. The respondent sometime to be nice towards the researcher to provides the wrong data. The respondent was unwilling to commit the fact that they were not hygienic. However, the agencies have worked a lot to aware the people regarding the use of the hygienic attitude in their daily behaviour. The collected day shows the successful knowledge impartation of the agencies in this area.

Figure 12: Knowledge of critical moments of hand washing
The collected data showed that around 26.1% of the respondents stated that they cleaned their hands after using the toilet. Further, only 23.3% of them commented that they washed their hands clean before eating. Around 16.5% of the people cleaned their hands before preparing foods and only 13.7% of them cleaned their hands after providing care to the sick people. It is analysed from the collected data that most of the people residing in the Somali region were not aware of the impact of not washing hands frequently.

Figure 13: What people use to wash their hands with
It has been analysed from the collected primary data that 58% of the respondents used Soap for cleaning their hands. Whereas there are around 20.2% of the respondents used ash for making their hands clean, and around 21.0% of the respondents used only water for cleaning their hands. It had been identified from the above data that most of the respondents were very reluctant to use basic hygiene. This seemed to be the main reason behind the outbreak of the AWD epidemic in the region of Somali in Ethiopia.

Figure 14: Where people in the family defecate
The primary data showed that around 64.9% of the respondents from the Somali region in Ethiopia routinely used the latrine for their family defecation purposes. About 29.8% of the respondents reported using the bushes to defecate. Further, 2.4% of the respondents used the area near the rivers for defecation purposes. The above data shows the importance of hygiene education for the people residing in the Somali region, and for the people to know that using an unhygienic means to defecate was/is harmful to their own health.

Figure 15: Why people in the family defecate in bush, river
It has been identified that around 30.9% of the respondents lack proper facilities of latrines so they are forced to use other alternatives and defecated in bushes and near the river body. Around 4% of the respondents stated that they do so because all the other members of the community did the same. The following of the tradition was/is one of the reasons behind the unhygienic means of defecation.

Figure 16: What people do with the faeces of small children?
The above figure shows 63.2% of the respondents during the period of data collection stated that they dumped their latrine. Further, 21.9% of the respondents buried their latrine. It was also analysed that 7.9% of the respondents stated that the dog ate the latrine. The lack of proper disposal of the faeces is/was the vital reason for the occurrence of AWD.
-
Knowledge: AWD spread
-
Practice: What people did when self or family member had AWD

Figure 17: Knowledge on how to get AWD
The awareness of the people residing in the Somali region was identified when around
37.9% of the respondents stated that using untreated water was the main reason behind the outbreak of the AWD. Further, 28.5% of them stated that eating contaminated food was the reason behind the occurrence of the AWD. While there were around 7.1% of the respondents who believed that the reason behind the spread of the AWD in the region of Somali in Ethiopia was due to the evil spirit. It can be easily analysed from the above data that the lack of proper awareness and knowledge regarding the reason for the occurrence of the AWD was due to the poor educational opportunities and a lack of proper facilities in their area.

Figure 18: If self or any member of the family has AWD in the past 3-6 months
The awareness level of the respondents was easily checked during the data collection process. It was identified that around 40.6% of the respondents’ family were suffering from AWD in the past 3 to 6 months, whereas 58.2% of the respondents commented that their family members were not suffering from the AWD in the last 3 to 6 months. It appears that the reduction in the proportion of people suffering from the disease of the AWD was due to the spread of awareness among the people with the help of the agencies like WHO and Red Cross.

Figure 19: What people did when self or family member had AWD
Data collected showed 44.5% of people consumed ORS when they are suffering from the disease of AWD, and 43.1% of the respondents go to the clinics for treatment. Only 11.7% of the respondents stated that they used traditional medical facilities in treating their family members from the AWD. It appeared from the data that the unavailability of the proper medical facilities is/was the basic reason for the small proportion of the respondents using the clinical facilities for the treatment of AWD.
-
What to do if one gets AWD

Figure 20: What would you do frequencies
The data analyses revealed 37.7% of people consumed ORS when they were suffering from the disease of AWD, and 45.6% of the respondents went to the clinics for the treatment. Only 7.1% of the respondents stated that they used traditional medical facilities in treating their family members from the AWD, and 7.5% stated that they preferred staying at home while suffering from AWD.
-
Knowledge on preventing AWD

Figure 21: Knowledge of how to prevent AWD
Analysis of data revealed 30.2% of the respondents stated that they believed that the main way to prevent the AWD was the treatment of the drinking water with chlorine. While 25.4% of the respondents stated that washing their hands can prevent AWD. The awareness regarding proper cleanliness is/was very poor among the people residing in the Somali region of Ethiopia. Hence, it showed that the respondent needed proper knowledge regarding the prevention of the AWD.
Nutrition-Related

Figure 22: How frequently do you breastfeed your child with diarrhoea or during illness
Analysis of the data revealed that 64.1% of the respondents commented that they very frequently breastfeed their children while suffering from the illness of AWD. Further, 17.6% of the respondents stated that the frequency of breastfeeding depended on the demand of the child. The above data very clearly showed the lack of knowledge and awareness of the respondents.
Knowledge related to Childs appetite

Figure 23: Knowledge of what to do during child sickness or appetite loss
Data analysis revealed 28% of the respondents believed that the appetite of the children will increase with the consumption of the soft drink. While 28% of the respondents, on the other hand, stated that child should be offered porridge during the illness period. Only 4.3% of the respondents stated that the child must be given spicy food to make them strong.

Figure 24: Knowledge-when child is sick
Analysis of data revealed 34.1% of the respondents believed that extra foods would help in curing the disease and 26.9% stated that the child must be given a proper liquid. Responses indicated 31.5% of the respondents thought that continuous breastfeeding was vital. Hence the respondents did not have proper knowledge regarding the diseases.

Figure 25: Has your child been screened by HEWs in the past 3 months?
Data indicated 68.5% of the respondents stated that their child was screened properly during the past three months; on the other hand around 31.5% of the respondents had a negative reply to the question. The proper screening and monitoring of the HEW are useful for the prevention of AWD, and education about this is needed based on the data analysis.

Figure 26: Knowledge on if SAM is a disease
Data analysis revealed 90.3% of the respondents had knowledge about SAM being a disease. This demonstrated the impact of the awareness through services from agencies and the government.

Figure 27: Knowledge on if SAM is treatable
99% of the respondents had knowledge regarding the treatment of the SAW. This data revealed the awareness of the people regarding the treatment of the SAM.

Figure 28: Knowledge of symptoms of SAM
Data analysis revealed 98.5% of the respondents had proper knowledge regarding the symptoms of SAM, whereas only 1.5% of them were unaware. It appears the proper speed of awareness by the government of Ethiopia was one possible reason behind this mass awareness.
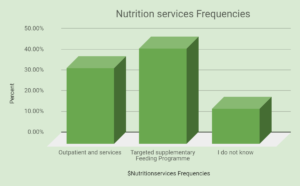
Figure 29: Nutrition services Frequencies
Analysis of data revealed 36.7% of the respondents had proper knowledge about the nutrient serviced to the patient during the illness. 46.2% believed in the feeding programmes, while 17% of the respondents were unaware. The above data clearly indicates that the people were ignorant about the facts and thus needed mass awareness about the proper intake of nutrients during illness.

Figure 30: Entitlement Frequencies
According to the collected primary data, most of the affected individuals were children under 5 years of age, while 35.5% of the pregnant mothers were affected by the diseases. And 8.6% of all the members of the community were affected by the diseases according to the respondents.

Figure 31: Do you think it is important to have your child vaccinated at health facilities or when a vaccinator comes to your home
Data analysis revealed 96.45 of the respondents stated that it would be beneficial if they were able to provide the vaccinations at home. This showed that the proper medical facilities were not easily available in the area and hence the respondents were unable to take their children for the proper vaccinations.
Figure 32: No vaccination Frequencies
Analysis of data revealed 10.3% of the respondents stated that they were not getting proper services, while another 10.3% of the respondents stated that they heard a rumour of the vaccine not being safe. Further, data indicated 30.9% stated that the vaccine might hurt their children, while 16.5% of the respondents stated that they thought the vaccine was of no use for the child. The above data clearly indicated the lack of awareness among the respondents.

Figure 33: Assets home Frequencies
Analysis of data revealed that 24.3% of the respondents had a TV in their home; 13.5% of the respondents had a dish connection to their TV; 31.3% of the respondents had a radio; 17.1% had a mobile phone; while 5.0% had the internet. The lack of proper global connectivity restricted the opportunities of the people to be informed and to grow properly in their awareness. Analysis of data revealed 4.7% of the respondents stated that they got information from their friends, and 7.3% of them stated that family was the main source of information for them. Further it was discovered that 8.9% of the respondents obtained information from their neighbours. Information through mobile phones and announcements were least methods available to them according to the respondents.

Figure 34: in the past 3 months have you heard any radio advertisement about AWD
Data analysis indicated 51.1% of the respondents stated that they had heard the advertisements on the radio regarding the AWD, while about 48.4% of them did not hear any such advertisements. The lack of proper mass communication strategies in the region was one important reason for the huge difference in both selected criteria.

Figure 35: Radio messages frequencies
Data analysis found 20.3% of the respondents stated that the advertisement was about the treatment of the water, while 17.2% stated that it was regarding the use of soaps. Further, 12.2% stated that the advertisements’ pertained to laws regarding cooking food well. Hence, the above data represents that mass awareness is/was very important for imparting proper knowledge among the respondents.

Figure 36: in the past 3 months, have you ever watched any TV advertisement about AWD
Analysis of data indicated40% of the respondents had seen an advertisement on TV regarding AWD, while 60% had not. The lack of awareness is/was clear as revealed in the analysis of the above referenced data.
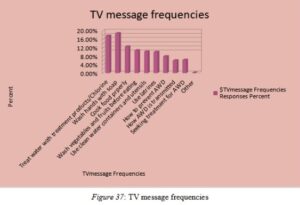
Figure 37: TV message frequencies
Analysis of data indicated 17.7% of the respondents stated that the advertisement was about the treatment of the water, while 18.8% stated that the advertisement was regarding the use of soaps. Further, 12.5% stated that the advertisement pertained to laws regarding cooking food well. Hence, the above data demonstrated that mass awareness is/was very important for imparting proper knowledge among the respondents with the help of television.

Figure 38: In the past 3 months, have you seen read any poster on AWD
Analysis of data revealed 54% of the respondents had seen a poster regarding AWD, and 46% had not. The lack of awareness is/was clear as portrayed in the figure of the data.

Figure 39: Poster message frequencies
Data analysis indicated 20.6% of the respondents stated that the advertisement was about the treatment of the water, while 18.5% stated that it was regarding the use of soaps. Further, it was found 12.1% stated that the advertisement pertained to laws regarding the cooking of food well. Hence, the above data illustrates that mass awareness is/was very important for imparting proper knowledge among the respondents with the help of poster messages.
Number of people who had seen any of the posters
The data analysis also noted 72.6% of the respondents had seen a poster regarding AWD, while 27.4% had not. Finally, analysis of data revealed only 72.2% had seen a poster regarding awareness. The lack of awareness was clear as illustrated in the above data.

Figure 40: Place of poster frequencies
Analysis of data found 37.6% of the respondents stated that they had noticed the poster on the wall of the clinic, while 18.8% said that the poster was seen by them on the notice board. Further, it was noted that16.1% of them were shown the poster by the HEW. The initiative regarding the awareness and education concerning AWD is/was very important, and subsequently educating the people residing in the area is/was of utmost importance.

Figure 41: People visited by a community worker/mobilize in the past 3 months
Out of 73% of respondents, 63.6% stated that they were visited by the community workers in the past 3 months, and 9.4% indicated that they were not served by the community worker in the last 3 months.

Figure 42: Transition of AWD
The respondents said that 22.6% of the discussion was based on the reasons and ways for the transmission of the AWD, and 20.1% of the respondents said that the discussion was regarding the prevention of AWD. Interesting it was noted 10.7% believed that the discussion was placed for the treatment of the diseases. The above data illustrates that the agencies must cover all the areas of discussion for the improvement of the knowledge of the respondents.

Figure 43: Work of CHW
Analysis of data revealed 32.3% of the respondents stated that the community worker demonstrated the poster on the AWD. While 31.7% stated that they demonstrated how to wash hands, and 32.7% said that CHW showed them how to prepare ORS. The data showed the contribution of CHW for the betterment of the people of the Somali region.

Figure 44: Have you taken part in any discussion about AWD in your community
Data analysis indicated 75.4% of the respondents were themselves taking part in the discussion over AWD, while 24.6% of the respondents kept themselves away from any such kind of discussions. The awareness could only be created among the people with the help of the mass participation of the people in the discussion regarding AWD.

Figure 45: Whole Frequencies
Analysis of data found 20.8% of the respondents said that the community discussion was led by religious leaders, and 32.2% stated that the health extension workers were the leaders of the discussions. Results indicated 31.5% stated it was the Kebele or government officers. Awareness is/was vital to reduce severe diseases. Data suggested here that the person leading the discussion must have a strong convincing personality.
Summary
Hence, it can be concluded by the analysis of the above data with the help of graphs that the lack of proper knowledge and awareness among the people were the main reasons for the outbreak of the AWD in the Somali region of Ethiopia. The lack of proper education and health facilities were also two important criteria in which they lacked miserably. The measures adopted for the purification of water needed modification. The primitive methods of water purification did not fit in the recent context. The identification of the disease in the early stage and care related to the treatment of the diseases was not adequate. The awareness practices were proving to be effective in the area. The region still needed more effective measures.
Hence, it can be concluded that the unhygienic situation would be very harmful to any society. They carry the potential to harbour the factors for various dangerous diseases. It is important for society to understand the importance of cleanliness and working together to overcome the AWD. The Somali region of Ethiopia suffered from the epidemic of AWD due to the rapid flood and creation of an unhygienic situation in the areas. The diseases were and continue to be the primary reason for the poor health conditions of the people of Somali. The lack of proper sewage systems, as the area is a drought prone area, is also considered to be a vital reason for the outbreak of the AWD. The lack of awareness among the people, as well as the scarcity of fresh and purified drinking water force the people to consume dirty water for survival. The low economic conditions of the people and the poor medical facilities available were and still are the main causes behind the outbreak of diseases like watery diarrhoea. It will continue to be vital for the citizens to have a basic sense of living a healthy life. Creating awareness is essential for the people residing there to live a healthy and diseases free life. AWD is a harmful disease and can be a threat to life if not treated at the correct time. It is necessary for the area of Somali to have proper access to medical facilities. The improvement of the available medical facilities can be beneficial for the native people of Somali. The proper availability of the medical facilities is very important for the country to overcome the severe epidemic. The lack of proper medical facilities in Somali was the main reason behind the causes of the severe epidemic and resulted in the loss of numerous people. The statistics of the people reported to be affected by the diseases was alarming.
Linking with Objectives
Objective 1: Health seeking behaviour of Ethiopia citizens from the Somali region
The medical health conditions of the people were very miserable in the Somali region of Ethiopia. The lack of proper medical facility made the government helpless in the situation of a severe outbreak of epidemic like in the case of the outbreak of the AWD. The tribes of Somali region were and continue to be mainly nomads surviving in the extreme climatic conditions. The Somali people believe then and now that the clan families are superior to that of the Saab. The hierarchy of the caste system is visible among the tribal groups as well. The living practice of the people varies from tribe to tribe and is unhealthy in nature. The unhygienic living conditions of the tribal people of Somali continue to be the root cause of the origination of the epidemic AWD. The situation of panic arises among the citizen during such a situation. The government of Ethiopia was forced to request the social welfare agencies to come forward in helping the people of Somali to survive this difficult situation. Social agencies such as Red Cross and W.H.O came forward to help the needy and save the lives of people fighting with the Watery diarrhoea. The agencies provided clean utensils and food for the people. They also provided bags consisting of ringer lactate. The increase in the number of the healthcare sector is badly needed by the region (Verguetet al. p.345-355). It has been observed that the region in the need of better medical facilities and safe drinking water to live a healthy life. It is high time for the government of Ethiopia to work to improve of the health care structure of the Somali region. The serious drawback in the proper medical structure can be noticed in the region, and the consequences were brutally highlighted during the outbreak of AWD as presented in this research study.
Objective 2: The extent of awareness, attitude shaping and seeking care regarding AWD among Somali region people
Creating proper awareness among the people of the Somali region of Ethiopia continues to be important. Until and unless the people of the region have access to proper knowledge about the benefits of living a healthy life, it will be very difficult for them to practice it. The proper maintenance of stationary health promoting conditions needs to be considered. Use of clean and safe drinking water is needed for the people of Ethiopia. The frequent flood in the Somali region has created an unhygienic situation and the people were forced to live in the poor environmental conditions. It has been observed that the flood leads to accumulation of the stagnant water for the long period of time and thus becomes the breeding ground for numerous diseases. The use of the proper disposal system by the citizens is needed to keep the climate clean and healthy. AWD remains a significant public health problem in many parts of the Somali region of Ethiopia, where disease can spread quickly unless an outbreak is stopped (Terfassa, 2015).
This underpins the international partners’ evidence on humanitarian responses to AWD in Ethiopia, in terms of necessary cross district and cross border coordination, as well as the human and financial resources needed. It has been identified that the creation of awareness among the people is vital and needs to be executed in an organised manner. It is an important task to convince people and encourage them to adopt healthy living habits.
Objective 3: The factors that have impacted the health seeking behaviour of Ethiopia region people
There were numerous factors that were responsible for making the health seeking behaviour of the People of Ethiopia region worse. The first and foremost is a natural calamity. It has been an analysis that the natural disaster plays an important role in making the health care of the entire area suffers. The repeated flooding in the region of Somali was a vital reason for the rise of the panicking healthcare scenario. It has been identified that the unavailability of the proper healthcare infrastructure contributed yet another factor for the poor health conditions of the people of the Somali region of Ethiopia (Seid et al. 2018, pp.236-241). The people residing in the Somali region of Ethiopia are primarily the economic weaker section of Ethiopia. The lifestyle of the people is not up to the mark. The food they intake is not healthy and thus they are unable support their immune systems from the numerous diseases. Poor sanitation conditions are also one of the vital reasons for the outbreak of epidemic diseases such as AWD.
Recommendations
The following recommendations are intended for the improvement of the healthcare system of the Somali region. It is vital for the people residing in the region and government of Ethiopia to work towards the betterment of the healthcare system of Ethiopia. Therefore, the following improvements are needed:
-
The increases in number of healthcare institutions in Somali region are needed for the up-gradation of the medical facilities available for the people residing there.
-
The creation of proper awareness among the people is needed for the improvement of the health of the people residing there.
-
The government of Ethiopia needs to allocate more funds to the healthcare sector of the country.
-
Improvement in the AWD detection machine is needed.
-
It is important for the government of Ethiopia to maintain proper sanitary situation among the area for Somali.
-
The government needs to work towards the improvement of the drainage facilities of the Somali area.
Limitations of the research
The execution of the research in an organised and systematic manner was not always possible. The researcher faced lots of difficulties and challenges in the proper execution of the research work. The researcher needed to overcome all the challenges and execute the best possible manner for the completion of the research study. The time limitations were one of the major issues faced while conducting the research. The collection of primary data was very vital and needed proper time to collect proper data by interviewing the people belonging to the different communities. It was very important for the researcher to execute his research-related activities in a planned manner. Proper planning was vital for the execution of the entire dissertation on time.
Language was a huge barrier. The people belonging to different communities had a different language. This made it very difficult for the researcher to convey their questions properly to the person when they were conducting an interview. The interview of five different communities with entirely different cultural beliefs and languages was a great issue faced during the data collection of the research. The unavailability of proper resources restricted the researcher from conducting proper research approaches. The sampling of the data was also a great challenge. The collection of the authentic data and sampling it properly needed to be done in a much organised manner. The collection of authentic data and making and the maintenance of privacy were vital. The privacy of the person needed to be respected by the researcher and it was important for them to let the interviewer maintain his own privacy. The researcher should not make the interviewer uncomfortable while collecting information from them. Adaptation of the proper data collection approach was needed for the researcher in the collection of the proper and authentic data. The resources available were also a huge restriction that the researcher suffered during the execution of the research study.
Future scope of the research
The research work presented in this dissertation shall be an important source of literature for the future research and shall provide a definite base for in-depth research studies. The research paper contains the detailed explanation of the factors contributing to the occurrence of the AWD diseases and the resource shall be an essential source of information for epidemics like that of AWD. The research study can also be an important source of awareness among the people regarding the maintenance of hygiene, latrine use, food handling and the impact of living in an unhealthy environment and household. The AWD tracking system needs to be more effective to identify the disease patterns at the early stages to detect, refer and or treat the citizens at the correct time. The development of rapid response teams shall be beneficial for the citizens of the Somali region of Ethiopia to fight against this epidemic and live a healthy life. Creating awareness and changing their point of view was the main reason for the conduction of the research work. Hence, the research study has numerous advantages as it contains vital information regarding the reaction of the people towards the severe epidemic disease like that of AWD.
REFERENCES
Alemayehu, L., Girma, S., Lemma, S., & Gatellier, K. (2018). How to improve child health
service utilization in Ethiopia.22(3). pp.56-69.
Azage, M., and D. Haile, (2015). “Factors affecting healthcare service utilization of mothers
who had children with diarrhoea in Ethiopia: evidence from a population-based national survey.” Rural & Remote Health 15.4. pp.23-36.
Bell, E., Bryman, A., &Harley, B., (2018). Business research methods. UK: Oxford university press, pp. 255-260.
Berhe, Hailemariam, Abadi Mihret, and GebreYitayih, (2014). Prevalence of diarrheaand
associated factors among children under-five years of age in Enderta Woreda, Tigray,
and Northern Ethiopia,International Journal of Therapeutic Applications, 31, pp. 32–
37.
Beyene, H., Deressa, W., Kumie, A., & Grace, D. (2018). Determinants of diarrhoea morbidity: The case of children under five years of age among agricultural and agro-pastoralist community of southern Ethiopia. Ethiopian Journal of Health Development, 32(1). pp.25-98.
Birhanu, A., & Ayalew, S. (2018). Indigenous knowledge on medicinal plants used in and around Robe Town, Bale Zone, Oromia Region, Southeast Ethiopia. Journal of Medicinal Plants Research, 12(16), 194-202.
Bozdayi, G., Altay, A., Yahiro, T., Ahmed, S., Meral, M., Dogan, B., … & Ahmed, K. (2016). Re-emergence of genotype G9 during a five-and-a-half-year period in Turkish children with rotavirus diarrhea. Archives of virology, 161(10), 2879-2884.
Bryman, A. & Bell, E., (2015) Business research methods. Oxford: Oxford University Press
Cohen, L., Manion, L., & Morrison, K. (2013). Research methods in education. Abingdon: Routledge.
Cdc.gov (2016), Communicable Diseases retreated on 7.3.19 Retreated from https://www.cdc.gov/immigrantrefugeehealth/profiles/somali/communicable-diseases.html
Cronin, A., Sebayang, S., Torlesse, H., & Nandy, R. (2016). Association of safe disposal of child feces and reported diarrhea in Indonesia: need for stronger focus on a neglected risk. International journal of environmental research and public health, 13(3), 310.
Dagnew, M., Tiruneh, M., Moges, F., & Tekeste, Z. (2012). Survey of nasal carriage of Staphylococcus aureus and intestinal parasites among food handlers working at Gondar University, Northwest Ethiopia. BMC public health, 12(1), 837.
Degebasa, Z. (2018). Under-Five Children DiarrhealStatusandAssociated Factors Among Implemented and Not Implemented Community-Led Total Sanitation and Hygiene in Yaya Gulele District, Ethiopia, 2017. Journal of Medical Research and Health Sciences, 1(02), 6-18.
Desai, S. N., Akalu, Z., Teshome, S., Teferi, M., Yamuah, L., Kim, D. R., … & Mesganaw, C. (2015). A randomized, placebo-controlled trial evaluating safety and immunogenicity of the killed, bivalent, whole-cell oral cholera vaccine in Ethiopia. The American journal of tropical medicine and hygiene, 93(3), 527-533.
Eshete, N., Abebe, B., and Gudina, T,(2015). Implementation of community-led total
sanitation and hygiene approach on the prevention of diarrheal disease in Kersa District, Jimma Zone Ethiopia.” Science Journal of Public Health3(5), pp.669-676.
Gebremedhin, S., Mamo, G., Gezahign, H., Kung’u, J., & Adish, A. (2016). The effectiveness bundling of zinc with Oral Rehydration Salts (ORS) for improving adherence to acute watery diarrhea treatment in Ethiopia: cluster randomized controlled trial. BMC public health, 16(1), 457.
Gedamu, G., Kumie, A., & Haftu, D. (2017). Magnitude and Associated Factors of Diarrhea among Under Five Children in Farta Wereda, North West Ethiopia. Quality in Primary Care, 25(4), 199-207.
Getachew, A., Guadu, T., Tadie, A., Gizaw, Z., Gebrehiwot, M., Cherkos, D. H., … & Gebrecherkos, T. (2018)“Diarrhea Prevalence and Sociodemographic Factors among Under-Five Children in Rural Areas of North Gondar Zone, Northwest Ethiopia.” International Journal of Pediatrics 2018 14(2). pp.56-96.
Gizaw, Z., Wondwoson, W., &Bikes, D., (2018). Acute malnutrition among children aged
6–59 months of the nomadic population in Hadaleala district, Afar region, northeast
Ethiopia. Italian Journal of Pediatrics 44(1), pp. 21-22.
Hassen, S., Haidar, J., & Bogale, A. L. (2018). Occurrence of diarrhea and utilization of zinc bundled with ORS among caregivers of children less than five-years in Addis Ababa, Ethiopia. Journal of Public Health and Epidemiology, 10(9), 348-355.
Hazel, E., Bryce, J., & IIP-JHU iCCM Evaluation Working Group. (2016). Perspective: On Bathwater, Babies, and Designing Programs for Impact: Evaluations of the Integrated Community Case Management Strategy in Burkina Faso, Ethiopia, and Malawi. The American journal of tropical medicine and hygiene, 94(3), 568.
Memirie, S. T. (2016). Scale-up of high impact maternal and child health interventions in
Ethiopia: equity, cost and cost-effectiveness analyses 45(6). pp. 22-32.
Memirie, S. T. (2016). Scale-up of high impact maternal and child health interventions i
n Ethiopia: equity, cost and cost-effectiveness analysespp. 52-56.
Mohammed, Ibrahim, et al. “Prevalence of diarrhoea causing protozoan infections and associated risk factors in diarrheic under-five children in Bahir Dar town, northwest Ethiopia: a paediatric clinic-based study.” Ethiopian Journal of Science and Technology 9.1 (2016) 25(5)pp. 15-30.
Negara, Edessa, Geritu Neuro, and MulugetaKebede.”Microbiological assessment of drinking water with reference to diarrheagenic bacterial pathogens in Shashemane Rural District, Ethiopia.” African Journal of Microbiology Research11.6 (2017) 6(50. pp254-263.
Mohammed, Mekonnen. Drug Susceptibility Pattern and Associated Factors among Under Five Children in Dire Dawa, Eastern Ethiopia. Diss. Haramaya University, 2015.
Osonwa Kalu, O., E. Eko Jimmy, and S. Ema. “Utilization of Oral Rehydration Therapy in the Management of Diarrhea in Children among Nursing Mothers in Odukpani Local Government Area of Cross River State, Nigeria.” American Journal of Public Health Research 4.1 (2016)5(2) pp.28-37.
Sahiledengle, Biniyam, FessahayeAlemseged, and Tefera Belachew. “Sanitation practice and associated factors among slum dwellers residing in urban slums of Addis Ababa, Ethiopia: A community based cross-sectional study.” (2018) 51(2). pp.56.
Sasikumar, J. M., MekonenWolditsadik, and MeseretChimdessa. Ethnobotanical Study of Traditional Medicinal Plants in Adami Tulu JidoKombolcha District, Oromia, Ethiopia. Diss. Haramaya University, 201815(5). pp.25-98.
Seid, Kassaye Wudu, and Belayneh DebasuKelkay. “The prevalence of diarrhoea and associated factors among children under five years in Ethiopia.” IJAR 4.9 (2018) 236-241.
Seid, Lubaba, et al. “Molecular detection of Enteropathogens from diarrheic stool of HIV positive patients in Gondar, Ethiopia.” BMC infectious diseases 18.1 (2018) 354.
Sekaran, U., & Roger, B. (2016). Research methods for business: A skill building approach.
Hoboken: John Wiley & Sons.
Shaw, B., Amouzou, A., Miller, N. P., Bryce, J., & Surkan, P. J. (2017). A qualitative exploration of care-seeking pathways for sick children in the rural Oromia region of Ethiopia. BMC health services research, 17(1), 184.
Shaw, B., Amouzou, A., Miller, N. P., Tsui, A. O., Bryce, J., Tafesse, M., & Surkan, P. J. (2015). Determinants of utilization of health extension workers in the context of scale-up of integrated community case management of childhood illnesses in Ethiopia. The American journal of tropical medicine and hygiene, 93(3), 636-647.
Singh, M., MrSephu, &, DoreshorK., (2016). Investigation on urban drainage systeminSululta
City, Ethiopia. International Journal of Engineering 8(1), pp. 1-10.
Tefera, G. (2015). Prevalence of intestinal parasitic infections among patients with diarrhoea at Wonago health centre, Southern Ethiopia: a retrospective study. Immunology and Infectious Diseases3(1), pp. 1-6.
Teferi, E., Tafessae, Z., & Ali, I. (2016). TRENDS IN HEALTH SERVICE UTILIZATION OF ICCM AND IMNCI IN FOUR REGIONS OF ETHIOPIA. Ethiopian Journal of Pediatrics and Child Health, 12(2), 13-20.
Tuem, K. B., Gebre, A. K., Atey, T. M., Bitew, H., Yimer, E. M., & Berhe, D. F. (2018). Drug Resistance Patterns of Escherichia coli in Ethiopia: A meta-analysis. BioMed research international, 2018.
Unicef.org (2016), UNICEF Somalia Annual Report 2016 Retreated on 7.3.19 Retreated from https://www.unicef.org/somalia/resources_20195.html
Unicef.org (2017), UNICEF Somalia Annual Report 2016 Retreated on 7.3.19 Retreated from https://www.unicef.org/somalia/resources_20195.html
Venkatesh, V., Brown, S.A. & Bala, H., (2015). Bridging the qualitative-quantitative divide: Guidelines for conducting mixed methods research in information systems. MIS Quarterly, 37(1), pp. 12-45.
Wamai, Richard G. (2014) “Reviewing Ethiopia’s health system development.” Population
(mil), pp.75-95.
Wang, H., Tesfaye, R., NV Ramana, G., & Chekagn, C. T. (2016). Ethiopia health extension program: an institutionalized community approach for universal health coverage. The World Bank. 5(65). pp 45-98.
Warsame, H. A. (2016). Influence of Health System Factors on Morbidity of Diarrheal Disease Among Children Under Five Living in Internally Displaced Population Camps of Hodan District, Mogadhishu. The Journal of Global Health Care System, 6(2).
WHO’S report on Somali. (2016). who.int. Available at: https://www.who.int/emergencies/crises/som/sitreps/en/ [Accessed on: 17/02/19
Woldie, H., Kebede, Y., & Tariku, A. (2015). Factors associated with anemia among children aged 6–23 months attending growth monitoring at Tsitsika Health Center, Wag-Himra Zone, Northeast Ethiopia. Journal of nutrition and metabolism, 2015.
Looking for best Dissertation Assignment Help. Whatsapp us at +16469488918 or chat with our chat representative showing on lower right corner or order from here. You can also take help from our Live Assignment helper for any exam or live assignment related assistance.